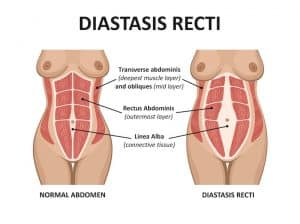
Diastasis rectus abdominis – also known as abdominal separation, is the widening of the gap between the left and right sides of your abdominal muscles. It can be painful and distressing (or not – my Dad has a diastasis but doesn’t find it troubling enough to do anything about it!) and it sometimes requires surgery. But how does it happen, and what can we do about it?
Anatomy – the abdominal canister
The abdomen is basically built like a can of beans, with the abdominal contents – your stomach, your intestine, your liver and all the other organs, plus your bladder and your uterus if you have one – kept firmly inside.
The top of the can is the diaphragm muscle, which basically forms the floor of the lungs and the roof of the abdomen, and the bottom of the can is the pelvic floor, which is there to stop everything falling out.
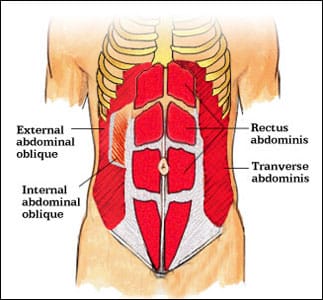
The cylindrical part of the can is formed by your abdominal muscles, of which you have three layers.
- The rectus abdominis is the six-pack muscle which sits at the front of your abdomen. The fibres run vertically down the abdomen, from the bottom of the ribcage to the top of the pelvis, and you have one on the left and the other on the right. When the rectus abdominus contracts, you bend forwards in the middle, like when you’re doing a sit-up.
- Underneath the rectus abdominis, the next layer of muscle is the obliques – external and internal. The oblique fibres run diagonally, up and down each side of your abdomen and their job is to help you twist, like when you’re doing a sit-up with a twist, or when you go to look over your shoulder as far as you can, or when you swing, like boxing or hitting a tennis ball. Again, you’ve got left obliques and right obliques.
- The deepest layer of abdominal muscles is the transversus abdominis fibres. Transversus’ fibres run more horizontally, so their job is to act a bit like a corset. They don’t produce movement, so much as when you contract the transversus abdominis, you squash your abdominal contents in a bit, so your tummy looks flatter. Again, you’ve got a left transversus and a right transversus.
In the middle is the linea alba, or white line, which is a sort of ligament. Its job is to transfer force between the two sides of the abdomen, especially between the left and right obliques, and the left and right transversus. You couldn’t twist forcefully, or flatten your abdomen forcefully, if you didn’t have a linea alba, because to produce movement, each muscle has to have two ends to pull on, and the linea alba forms one end. So when you twist to the left, it’s because your right external oblique muscles pull on the linea alba, and so your right shoulder moves towards the midline of your body. If the linea alba wasn’t there, your right external oblique muscles couldn’t produce any force as they’d have nothing to pull on.
Diastasis Rectus Abdominis (DRA)
That’s where DRA comes in. In some people, and it’s usually people who’ve gained a lot of weight around the tummy or who’ve been pregnant, the linea alba can get overstretched. That’s what we call a diastasis, or gap. And once it’s been overstretched, it often doesn’t ping back by itself when you lose the weight or have the baby – instead, it goes a bit soft and floppy, like an overstretched elastic band. You might see a gap, or be able to sink your fingers through it.
A diastasis causes functional problems because you can’t use your abdominals properly when you don’t have anything to pull on. It also means that the abdominal contents often aren’t held in properly, so your organs can start poking through the gap and falling forwards – which doesn’t look very nice but is also super uncomfortable. It also means that the abdominal canister doesn’t work very well, which can have knock-on effects for your diaphragm and your pelvic floor, so you can end up with breathing problems, reflux and incontinence, prolapses, back pain, pelvic pain and sexual problems both physical and psychological. Oh, and it puts you at greater risk of hernias – inguinal (at the groin or pelvic floor), abdominal (usually somewhere along the linea alba) and hiatal (at the diaphragm). So although a diastasis is often considered just a cosmetic problem – and unfortunately that’s essentially how the NHS looks at it,– it can actually have really serious consequences.
So, how wide should the linea alba be, and how do you know if you’ve got a diastasis?
In 2009, Beer et al used ultrasound imaging to investigate the width of the linea alba in 150 healthy women between the ages of 20 and 45, who had never been pregnant. The gap between the left and right rectus abdominis was measured at three points along the linea alba: at the xiphoid, 3 cm above the umbilicus and 2 cm below the umbilicus. They found high variability at all three levels and reported the mean width to be 7mm ± 5 at the xyphoid, 13mm ± 7 3cm above the umbilicus and 8mm ± 6 2cm below the umbilicus. Anything wider than these were considered abnormal.
But abnormally wide doesn’t necessarily mean problematic, by itself.
You see, the other important thing about the linea alba is that it should also feel firm all the way along its length, except for right around your belly button. So you shouldn’t be able to sink your fingers into it, it shouldn’t feel soft and floppy.
So an abnormally wide linea alba becomes a problem when you can’t use it functionally, can’t generate force across it because it’s too floppy.
A test we use to see how functional your linea alba is, is something we call the curl-up task. Essentially, you lie on your back with your knees bent, and you lift your head towards the ceiling.
We measure the width of your linea alba in the three places – top, middle and bottom. We do this
- at rest,
- when you’ve lifted your head far enough that your shoulderblades are starting to lift, but without giving you any more instructions than that
- when you’re in the curl-up position, but before you started, we asked you to contract your transversus abdominis, the corset muscle.
What should happen is that your linea alba should stay the same width, irrespective of whether you’re resting, or curled up, or curled up with a cue.
In people with a dysfunctional diastasis, this doesn’t happen. What tends to happen with people who have a dysfunctional linea alba, is that the linea alba gets narrower and floppier as you lift your head. So if you can only sink your fingers a little way into it when you’re at rest, then if your linea alba is dysfunctional, when you lift your head, you’ll be able to sink them in further. Or, you may find that instead of being able to sink your fingers in, your abdominal contents push up and through, creating a dome shape.
However, that’s not the end of the story. Some people with a dysfunctional diastasis will respond to exercise, and others won’t, and we need to work out which one you are likely to be.
So we use a cue, which means that we tell you to switch on your transversus abdominis muscle (your corset muscle), before you do the curl-up task.
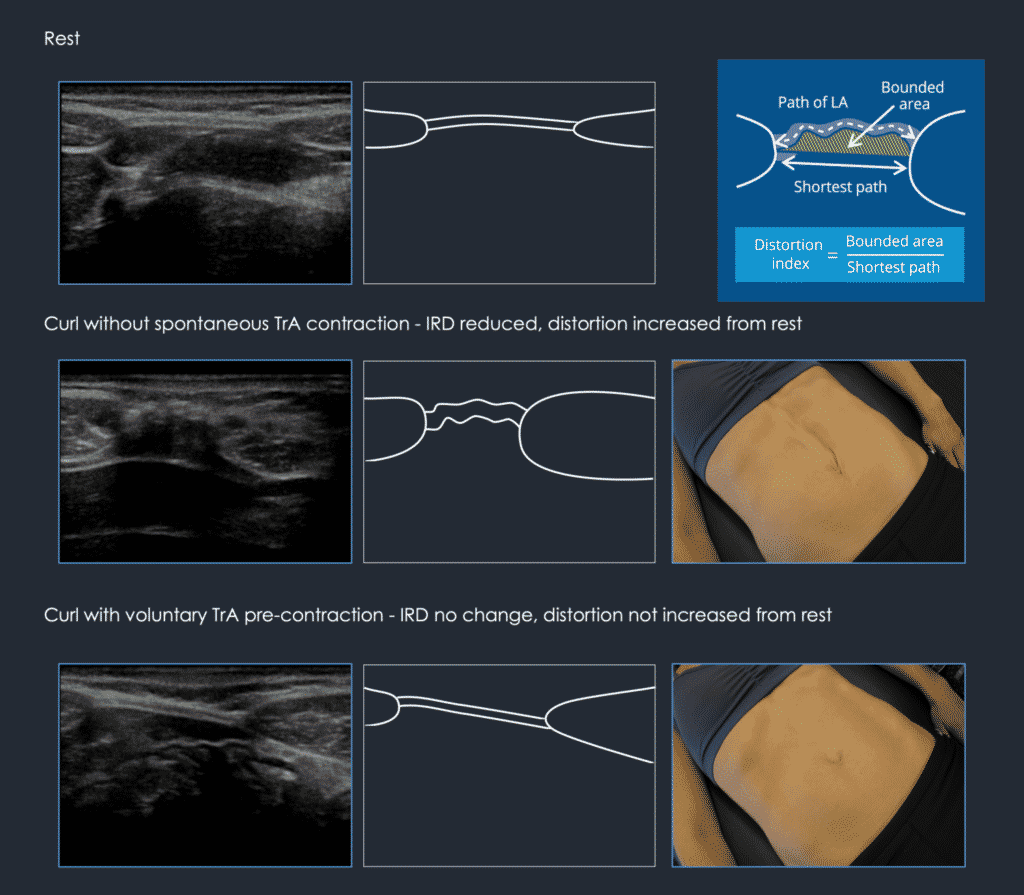
This slide, taken from Diane Lee and Paul Hodges’ 2016 research paper in JOSPT, shows what happens to someone who has a diastasis, but who can control it.
At rest – the top diagram, which is a tracing of the ultrasound scan on the top left so that it’s a bit clearer – you can see the linea alba in the middle, between the two rectus abdominis muscles. Although it’s too wide, it’s nice and taut.
In the second diagram, the patient has been asked to lift her head up with no other instructions. We know she has a diastasis, because the rectus abdominis muscles have moved closer together, and you can see that the linea alba has gone wiggly and soft, instead of taut and stretched. In this situation, you might either see a sort of groove forming in the linea alba, or you might see doming, with the abdominal contents pushing through the gap – but either way, it’s soft and you could sink your fingers into it.
But the third diagram is the important one. In that diagram, the patient was asked to switch on her transversus abdominis before lifting her head, and we can see that the linea alba has stayed taut and stretched, the same as it was in the first diagram. This means that she can generate force across the linea alba, which is a really good sign as it means she will respond to the right type of exercise treatment.
When transversus abdominis pulls on the sheaths of the recti muscles and then the linea alba (thus pulling it wider) it also reduces the distortion. In other words, the midline doming or sagging is less and the abdomen appears flatter because the TrA muscle is pulling everything in. The goal is not to reduce the diastasis after all – it is to widen it, load it, and hold the abdominal contents in!
If the third diagram didn’t look like that, if the linea alba stayed floppy and wiggly, then it would be a different situation. If we couldn’t train her to generate tension across the linea alba – and that could be because the connective tissue is too floppy, or because there’s something interrupting the signals between the brain and the abdominal muscles, or because there’s a hernia – then we’d be thinking more on the surgical side of things, and starting to talk about a repair.
So ultimately, what’s important is not the width of the diastasis, but whether you’re able to generate tension across it so that you can use it like a normal linea alba.
How do you cue the transversus abdominis?
Getting the transversus abdominis to create tension across the linea alba can be an interesting challenge, because different people respond to different cues. The trick is to find the right cue for the individual.
Common useful cues include:
- Try to lift your pelvic floor (if you know what that is!)
- Imagine you are trying to suck something up into your vagina (if you have one)
- Imagine you are trying to shorten your penis (if you have one)
- Imagine you are trying to stop yourself from urinating
- Squeeze your back passage
- Imagine you are walking into a very cold lake, and the water is at mid-thigh and you are trying to go as deep as you can without getting your genitals wet!
- Try to tense your lower abdominals
- Try to flatten your belly button against your spine
If you’re struggling to activate the transversus abdominis with any of these cues, we may assess you to find out if there is a physical issue that’s inhibiting it, using the Integrated Systems Model to identify a driver. If we find that an area of the body – for example, the neck, thorax or pelvis, is out of alignment and inhibiting the transversus abdominis, then we can correct the driver and then cue your muscle activation.
We test which cue is most useful by feeling the linea alba! When you find the right cue, the linea alba will get tauter and less floppy. You won’t be able to sink your fingers through it and you won’t get any doming as the abdominal contents poke through the gap. The diastasis may even get slightly wider – but it certainly won’t get narrower!

Once you can generate force across the linea alba with the transversus abdominis, then you can start to train it. When it’s taught well, Pilates-type exercise can be very useful for this, and the focus should be on controlling the linea alba rather than on trying to achieve a magic number of sets or reps.
What about sit-ups and planks? Are they dangerous?
This is a question that people ask a lot! Some doctors are very averse to the idea of people with a diastasis doing abdominal exercises such as sit-ups and planks. But – done properly, by people who are able to generate some tension across the linea alba – they can actually be quite useful.
I think the first question is, do you need to do sit-ups or planks, and if so, how many? And the answer is, it depends. When I was in the Army (because I was an Army officer for 14 years) I needed to be able to do sit-ups because twice a year we got tested on how many we could do in 2 minutes. So it was important for my career that I was able to do 55 sit-ups in two minutes!
Now, most people do not need to be able to do 55 sit-ups in 2 minutes, but it is useful to be able to sit up from lying down. If you’re healthy, you should be able to do that in lots of different ways, one of which is starting lying flat on your back, and then using your abs to sit up. That’s functional. Doing lots of sit-ups though, is probably less so!
However – whether sit-ups are dangerous or bad for you if you have a diastasis, is a different question. But the answer is still that it depends! It depends on whether you can control your linea alba. If you can control your linea alba, and keep creating tension through the linea alba throughout a sit-up, so that it doesn’t get narrow and floppy, then you’re safe to do a sit-up. If you can’t control your linea alba all the way through, then it’s something you should work on, and only go as far as you can control. If that means barely lifting your head in a curl-up, or barely lifting your foot, then that’s fine – that’s the level you’re at, and the level you need to work from. Sit-ups aren’t a bad exercise per se, but it’s easy to do them badly, and if you do too many sit-ups without good abdominal control, then you do put yourself at greater risk of injury – just like you would if you tried to run a marathon without doing so much as a jog round the block beforehand.
A plank by itself isn’t a very functional exercise either – but it’s useful to learn to control your linea alba in a plank position, because it is a similar position to the one we get into when we reach across for things. So if you can learn to generate tension across your linea alba at all, then I believe that learning to do so in a plank position is beneficial. But unless you need to do so for any specific reason, I don’t think there’s much point trying to set a planking world record!
And if I can’t generate tension across the linea alba, do I need a surgical repair?
Maybe. And if you do need a surgical repair, it needs to be functional, not just cosmetic, so that you can use your abdominal muscles again. The idea is to give the muscle something strong to pull against. You don’t want the repair to give way as soon as you try to sit up in bed!
I am not an expert on muscle repair surgery, but from the studies I have read and lectures I’ve attended, it seems to be important that there are at least two layers of stitches holding you together – at the front and at the back of the linea alba. If you have a hernia (a hole) or if your connective tissue is of very poor quality, then adding a mesh can provide a further layer of security to the repair.
However, before you go down this route, it is sensible to see a physiotherapist who is trained in treating people with diastis, to see whether it is possible to train your muscles to generate tension. There are risks associated with any surgery, and if you can avoid them, then I think it’s generally preferable! Equally, having a muscle repair operation will not magically restore the function of your abdominal muscles, so after the operation is another sensible time to see a physiotherapist who can help you to restore normal function of your abdominal canister, so that your diaphragm, pelvic floor, abdominal organs and spine are supported as effectively as possible.